He even went through periods where he could not walk properly – CK
 I’ve been told personally that a little gluten never hurt anyone. Clinical experience proves otherwise. The combination of misunderstanding, ignorance and rise in everything pervasively gluten-free has made the topic seem like a modern day fad. Unfortunately, this phenomenon affects those most for whom gluten sensitivity is a real, clinical issue.
I’ve been told personally that a little gluten never hurt anyone. Clinical experience proves otherwise. The combination of misunderstanding, ignorance and rise in everything pervasively gluten-free has made the topic seem like a modern day fad. Unfortunately, this phenomenon affects those most for whom gluten sensitivity is a real, clinical issue.
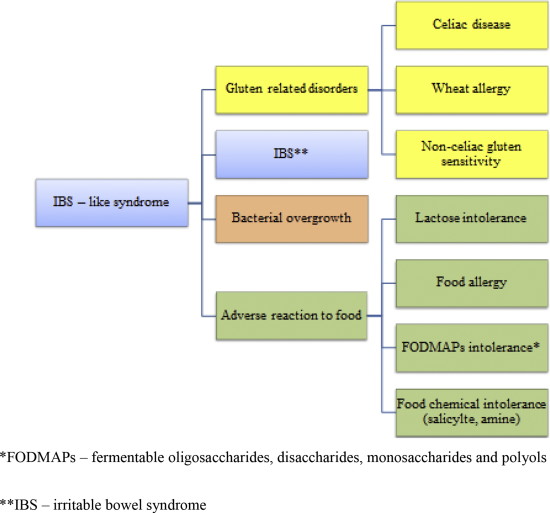
It is now becoming clear that, besides those with coeliac disease or wheat allergy, there are people with gluten sensitivity in whom neither allergic nor autoimmune mechanisms can be identified1. It has been estimated that for every person with coeliac disease there should be at least 6 or 7 people with non-coeliac gluten sensitivity (NCGS)1. In 2011 in London, a panel of 15 experts announced a new classification of gluten-related disorders (see yellow boxes below) that was then published in February 20122. The Second Expert Meeting on gluten sensitivity that was held in Munich in 2012, decided to change the name of gluten sensitivity to non-coeliac gluten sensitivity in order to avoid confusion with coeliac disease3.
The challenge with diagnosing NCGS is that currently there are no laboratory biomarkers specific for gluten sensitivity and the diagnosis is based mainly on exclusion criteria: elimination of gluten-containing foods from the diet and monitoring symptoms. Occasionally people will say they have attempted a gluten-free diet, yet symptoms persist. The problem with this is, firstly, foodstuffs nowadays are a complex minefield of chemicals and people may exhibit cross-reactivity with other wheat-based molecules and, secondly, the person may not have been strict enough with the diet or persisted long enough to heal the gut. Being completely gluten-free is incredibly challenging and often too difficult, so alternative diagnoses to gluten sensitivity are sought and the underlying issue is missed.
Many people that are intolerant of gluten are also intolerant of other proteins found in foods like dairy, eggs, and even coffee and milk protein. Critics of the gluten-free diet argue that people with irritable bowel syndrome (IBS) are not sensitive to gluten, but instead are reacting to a group of poorly absorbed carbohydrates called FODMAPs4 (figure below). From a practical perspective, wheat and many other gluten-containing grains are FODMAPs and should be avoided by people with gluten sensitivity anyway.
Coeliac disease is easier to diagnose than NCGS. Most doctors today know how to screen for coeliac disease. They will typically test for antibodies to alpha gliadin, transglutaminase-2, deamidated gliadin, and endomysium, and if positive do a biopsy to determine if tissue damage is present. However, we now know that people can (and do) react to several other components of wheat above and beyond alpha gliadin, the component that is implicated in coeliac disease. These include other epitopes of gliadin (beta, gamma, omega), glutenin, wheat germ agglutinin (WGA), gluteomorphin, and deamidated gliadin5,6.
The bottom line is standard blood tests by general practitioners are not comprehensive enough. The person may be reacting to deamidated gliadin, glutenin, gluteomorphin, and either transglutaminase-3 or -6, but not reacting to alpha gliadin or transglutaminase-2 (the antibodies used to screen for coeliac disease by most doctors). They will remain undiagnosed and continue to eat gluten for the rest of their lives, suffering symptoms and putting themselves at serious risk for autoimmune diseases.
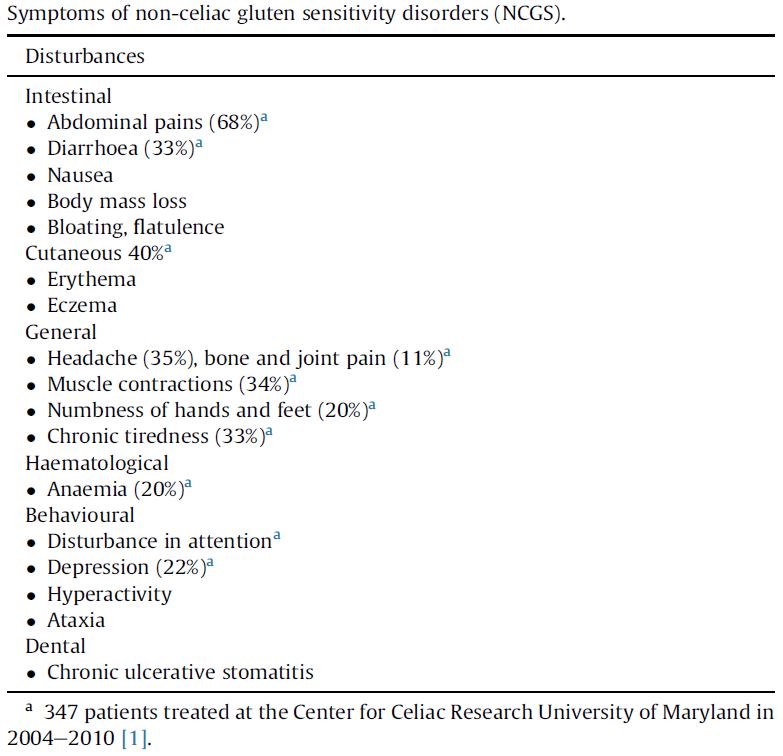
The typical presentation of NCGS is a combination of IBS and systemic manifestations like headache, joint and muscle pain, muscle contractions, leg or arm numbness, chronic fatigue, “brain fog”, body mass loss and anaemia. Symptoms can also include behavioural disturbances such as changes in attention or depression2 (Table of NCGS symptoms).
{kind=link}
IBS can include abdominal pain, nausea, bloating, flatulence, diarrhoea or constipation. People with IBS who respond well to a gluten-free diet can suffer from one of the three diseases: coeliac disease, wheat allergy or NCGS, where NCGS is the most likely option (figure above). In children, NCGS manifests with intestinal symptoms – abdominal pain and chronic diarrhoea – but also symptoms beyond the gut.
Extragastrointestinal manifestations seem to be less frequent but the most common is chronic tiredness. When a person with NCGS consumes wheat or other gluten-containing foods, he or she may not always experience the classic digestive symptoms associated with gut because they do not produce antibodies to transglutaminase-2 (which is mostly expressed in the gut). Instead, the intolerance of wheat may manifest in skin conditions like eczema or psoriasis; and in neurological or brain-related conditions like depression, peripheral neuropathy (pain, numbness, burning, tingling), ataxia (difficulty walking) or ADHD7. Current evidence suggests that neurological manifestations are immune-mediated and that there is cross-reactivity between immune cells, nerve cells and gluten proteins.
Gluten sensitivity is a common disorder that manifests in diverse ways, making it a difficult condition to diagnose. Many people who present with neurological manifestations of gluten sensitivity have no gastrointestinal symptoms7 ?
My son had been suffering from ongoing headaches, as well as a number of other symptoms, for years. Those symptoms included anxiety and periods of numbness in his arms and legs and difficulty sleeping and staying asleep. His learning ability, general demeanour and attitude to life was deteriorating. He went from being a cheerful, loving child to being withdrawn, depressed, moody and always off school sick. He even went through periods where he could not walk properly.
We were horrified when, after deciding to make a headache diary, we learned that he was having on average 8 headaches a day.
We spent a lot of time and money at various medical practices, with different medical specialists trying to get to the bottom of what was going on. My son was subjected to a large number of different medical tests. We even took him to Australia to see a medical specialist.
It made us extremely sad, not only to know that our son was suffering, but also that we couldn’t help him by finding the answer to what was going on. He just seemed to keep getting worse and worse.
Coming to Spinewave changed not only our son’s life, but also our life together as a family, as once our son started to get well, the stress on our family life lifted.
It did take some time but eventually our son recovered, and we are so grateful for this. As an aside to what Spinewave deals with on a day to day basis it was only Dr Neil Bossenger who picked up (where other doctors had not) that our son might have issues with gluten.
CK mother of 11 year and lawyer Auckland
References:
- Rostami, K. Non-coeliac gluten sensitivity. BMJ. 2012. 345:e7982.
- Czaja-Bulsa, G. Non coeliac gluten sensitivity – a new disease with gluten intolerance. Clinical Nutrition. 2015. 34(2): 189–194.
- Catassi, C., et al. Non-celiac gluten sensitivity: the new frontier of gluten related disorders. Nutrients. 2013. 5:3839e53.
- Biesiekierski, J., et al. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology. 145(2): 320 – 328.
- van de Wal, Y., et al. Glutenin is involved in the gluten-driven mucosal T cell response. Eur J Immunology. 1999. 29: 3133–3139.
- Vader, W., et al. The gluten response in children with celiac disease is directed toward multiple gliadin and glutenin peptides. Gastroenterology. 2002. 122(7): 1729 – 1737.
- Hadjivassiliou, M, et al. Gluten sensitivity: from gut to brain. The Lancet Neurology. 2010. 9(3): 318 – 330.
© 2015 Spinewave