 This case is the hallmark of having a progressive, working diagnosis and not getting stuck on one idea.
This case is the hallmark of having a progressive, working diagnosis and not getting stuck on one idea.
Disease processes can progress rapidly and any hunch or potential red flag should warrant reexamination, a second opinion, blood tests, or new imaging such as X ray or MRI.
The patient presented with years of chronic right sacroiliac pain, numbness and tingling down the back of the leg, and difficulty lifting things. My concern at the time she presented for care was the recent onset of urge incontinence in the last year, which up until this time was only being treated by injection.
The underlying cause was more sinister – as was the cause under that cause.
Sometimes the symptoms of chronic back pain and changes in bowel and bladder function can be tied together by cauda equina syndrome, which is extreme pressure on the nerves of the lower spinal cord. If cauda equina syndrome is not dealt with appropriately, sometimes immediately by surgery, there can be permanent damage to the nerves that control the legs, bowel and bladder.
Other concerns the patient had were inability to lose weight, thinning hair, thinning skin that frequently got damaged and didn’t heal quickly, a change in facial colour and osteoporosis.
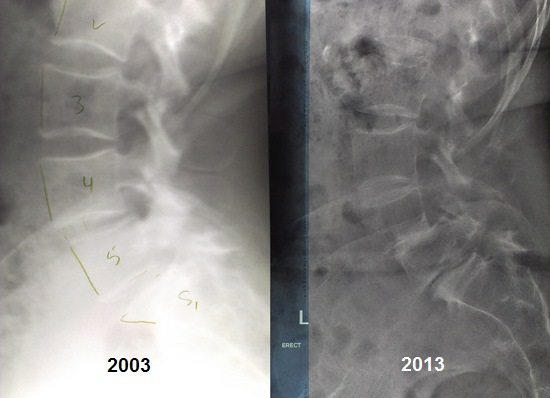
Initially, the patient gave me X rays from 2003 that were relatively normal (left). So the working diagnosis for the loss of bladder control was neurological at first. Whilst on holiday, she had a fall and the pain became progressively worse. I ordered a new set of films, shocked to find a double spondylolisthesis (right). A spondylolisthesis is the forward slipping of one vertebra on top of another. This process had occurred significantly over a 10-year period and was beginning to affect the function of the spinal nerves that controlled the patient’s bladder. It also accounted for the tremendous pain she was experiencing in her back and sacroiliac joint (hip).
I referred the patient to an orthopaedic surgeon for further investigation and an MRI. The first surgeon she saw suggested that this problem had probably been with her since childhood. The above X rays proved otherwise, so I suggested she seek another opinion.
Further testing revealed high levels of cortisol, which marked the beginning of the chief diagnosis and real underlying cause of all her health problems: a tumour on the pituitary gland, resulting in Cushing’s disease.
 A pituitary tumour tells the adrenal gland to pump out more and more cortisol, which is the same stuff stress is made of. Cushing’s disease (as opposed to Cushing’s syndrome) is difficult to differentiate from people under major stress or those taking lots of asthma medication because they may exhibit the same bodily signs.
A pituitary tumour tells the adrenal gland to pump out more and more cortisol, which is the same stuff stress is made of. Cushing’s disease (as opposed to Cushing’s syndrome) is difficult to differentiate from people under major stress or those taking lots of asthma medication because they may exhibit the same bodily signs.
However, when cortisol levels become high enough, certain signs and symptoms become significant: Bruises, long term abdominal obesity, fullness of the face, facial hair and acne, purplish linear markings on the lower abdomen and gluteal region, weakness and fatigue, limb weakness, thin skin, loss of memory and bone degeneration.
Long term stress and cortisol has detrimental affects on overall health for 4 reasons.
Physical, emotional and chemical stress, as well states of constant pain, tell the adrenals to produce more cortisol. Over time excess cortisol does 4 things:
- Stress depresses cartilage and bone formation, leading to osteopenia and osteoporosis.
- Stress inhibits inflammation, which is a bad thing because wounds don’t heal.
- Stress depresses the immune system, lending one to chronic illness.
- Stress causes changes in heart, nerve and gut function, leading to all sorts of issues.
After many working diagnoses and eventually finding the cause, the patient was referred for surgery to remove the pituitary tumour. We wish her a speedy recovery ?
 I was referred to Neil initially for a neck adjustment. I had long been cynical about the value of chiropractic but agreed to give it a go.
I was referred to Neil initially for a neck adjustment. I had long been cynical about the value of chiropractic but agreed to give it a go.
Neil began by checking me out as whole and noted areas that needed serious work. I was impressed that he also spent quite some time on the weekend researching my case!
For years I have had intermittent pain in the right sacroiliac area. I had also been experiencing urge incontinence episodes with my bladder and Neil wondered if that was connected with my spinal troubles, as spinal damage occasionally affects the spinal cord. I was reluctant to accept this but Neil was concerned about cauda equina syndrome and continued to check my spine, sometimes giving great relief after treatments.
The two-bed approach was a bit strange at first, but in fact, made me feel more in touch with what he was doing as I was aware of other people’s successes as he worked with them. He was always willing to explain what he was doing and why; his caring attitude was impressive.
Eventually, after some weeks of improvement, I had a fall which exacerbated my pain. Neil became even more concerned and ordered a new X ray, which was quite a shocker. I had a double spondylolisthesis! Neil referred me to a spinal surgeon who only recommended conservative care for my spine; however Neil suggested getting a second opinion and more tests.
At last after weeks of tests I had a definitive diagnosis of Cushing’s disease, which is pretty rare and potentially fatal. Well, that is if it’s not treated. I was to have a five hour operation on July 16th to remove a tumour on my pituitary, which hopefully will sort things out. It accounted for things like my round face, funny hair, osteoporosis, inability to lose weight no matter what, lack of strength and so on.
The surgery is all over now and the surgeon is very happy and optimistic.
Dorothy
© 2014 Spinewave